Think biG!
Urge- Intelligence
Insight. Intelligence. Impact
Development Intelligence & Insights
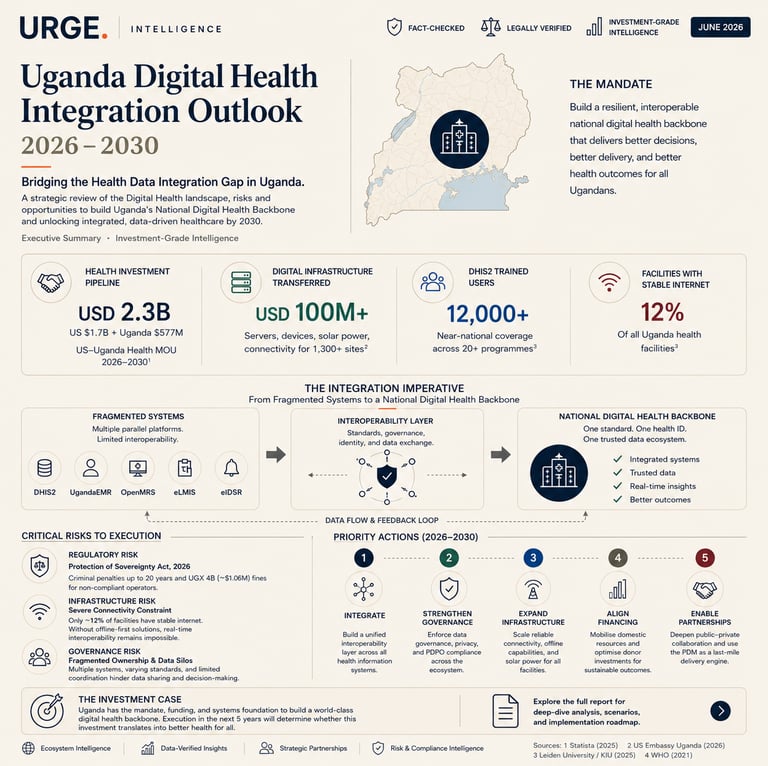
Bridging the Health Data Integration Gap in Uganda.
Release Date: June, 2026
Country: Uganda
Download & Read Full Report
This brief is free. Enter your email to download the full report, and development intelligence.
Urge- Intelligence
Dev- News
Urge Skill-Up
Knowledge is power.
Stay connected. Be informed.
© 2026 All rights reserved.
East Africa's Development Communications Institution.
© Urge Communications 2026
UrgeDevWire
Our Platforms
Informing. Inspiring. Connecting. East Africa's development community.